24 Feb. 2026 /Mpelembe Media/ — This research explores the profound intersections between intense romantic love, debilitating grief, and clinical addiction. By examining these human experiences through psychological, neurobiological, and sociological lenses, a unified framework emerges: both obsessive love and prolonged grief are dysregulations of the brain’s fundamental reward and attachment systems.
Why Your Brain Thinks Love is a Drug (and Grief is a Withdrawal)
The language of human attachment has long borrowed its vocabulary from the lexicon of pathology and affliction. Two millennia ago, Ovid lamented in his Amores , “I can’t live with or without you”—a sentiment echoed by the desperate modern refrain of “I wish I knew how to quit you.” For centuries, we dismissed these as mere metaphors for the intensity of the human heart.However, the current neurobiological paradigm shift suggests that these expressions are not poetic hyperbole, but precise descriptions of biological reality. Empirical data increasingly erodes the distinction between romantic attachment and substance dependency. Science is revealing that the “love sickness” of infatuation and the agonizing “withdrawal” of grief are not just like addiction; they are underwritten by the same neurochemical cascades and the recruitment of identical brain regions.
The “Broad View”: We Are All Technically Addicts
In clinical discourse, two primary frameworks define the relationship between love and addiction. The “narrow view” is the traditional medical model, suggesting that love only becomes an addiction when it elicits abnormal patterns of function—resulting in toxic, compulsive, or destructive behaviors. In this view, love addiction is a rare pathology.Conversely, the “broad view” posits that all romantic love exists on a “spectrum of motivation.” From this perspective, addictions are simply appetites: felt needs that become urgent when unfulfilled. This view suggests that even “normal” social attachment is a form of constructive addiction that evolved to facilitate pair-bonding and survival. While drug use “hijacks” these survival mechanisms, the underlying neural substrates remain the same.“By nature we are all addicted to love … meaning we want it, seek it and have a hard time not thinking about it… there is nothing dysfunctional about wanting love.”By shifting the focus from a “narrow” diagnosis to this broader spectrum, we recognize that the human brain is essentially designed for attachment. The question then moves from whether one is “addicted,” to whether a specific attachment enhances or diminishes one’s flourishing.
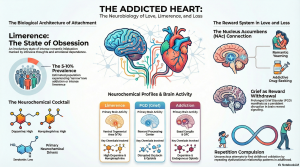
Limerence: When Infatuation Mimics OCD
The initial, involuntary stage of falling in love is often termed “limerence,” a concept defined by Dorothy Tennov. This state is characterized by intrusive thinking and a desperate yearning for reciprocation. In this phase, the brain undergoes a radical neurochemical shift: dopamine and norepinephrine surge, creating euphoria and heightened alertness, while serotonin levels drop precipitously.This specific drop in serotonin provides a neurochemical signature identical to that found in Obsessive-Compulsive Disorder (OCD). This explains the “Social Salience Hypothesis”—the involuntary, obsessive preoccupation with the “limerent object.” For the patient, this data validates the feeling of “losing control”; their brain is quite literally prioritizing the target of their affection with the same intensity an obsessive mind prioritizes a compulsion.
Grief as a “Reward Disorder”
If love is the biological “high,” then grief is the physiological “crash.” Recent systematic reviews of Prolonged Grief Disorder (PGD) suggest it is far more complex than simple sadness. PGD is better understood as a disruption of the brain’s reward system.When a loved one is lost, the bereaved experiences an “approach-avoidance” conflict. The brain’s reward center, specifically the nucleus accumbens (NAc), continues to “crave” the reward of the attachment figure (approach), while the amygdala processes the emotional salience of the loss and the subgenual anterior cingulate cortex (sgACC) drives ruminative yearning.This creates a failure of the prefrontal cortex (PFC) to regulate the craving. Yearning, in this context, is a neurobiological craving for an attachment figure who is no longer there to provide the chemical reward. The bereaved person is essentially trapped in a state of chronic withdrawal, where the brain’s reward signaling is persistently dysregulated.
The Rise of “Anti-Love” Biotechnology
The biological similarity between pathological attachment and substance use has led to the controversial prospect of pharmacological “cures” for a broken heart. Researchers are exploring the use of Naltrexone—an opioid antagonist typically used to treat heroin and alcohol addiction—to disrupt the “reward” of grief.Anecdotal clinical cases suggest that naltrexone can rapidly reduce PGD symptoms. In several instances, home-bound patients who were unable to stop viewing mementos of the deceased were able to move forward within days of treatment. However, as a neuropsychologist, I must emphasize that the ethical application of such “anti-love” biotechnology must meet four stringent conditions:
- The love or grief in question must be clearly harmful and destructive to the individual.
- The patient must provide explicit, informed consent.
- The technology must help the person align with their “higher-level” goals (e.g., returning to work or parenting).
- It must be psychologically impossible to overcome the pain through non-biological means.The goal is not to medicate away the human experience, but to restore autonomy when the biological “drive” has become a prison.
The “Why”: We Repeat What We Don’t Repair
Beyond the neurotransmitters lies the deeper psychological question of why we choose our specific “addictions.” Psychoanalytic theory suggests a conflict between the “Pleasure Principle” (the search for immediate gratification) and the “Death Drive” (or Nirvana Principle). The Nirvana Principle is a psychic force striving for a “tranquil state” by binding excitation and silencing the halls of the psyche.This often manifests as “Repetition Compulsion”—the tendency to unconsciously seek out love objects that mirror significant, often painful, figures from our childhood. We repeat these maladaptive patterns in a search for “abreaction” or mastery over a situation that once overwhelmed us. As the literature suggests, “the less we understand, the more we repeat.” We act out because we cannot yet remember or work through the original wound.
Conclusion: Toward a New Science of the Heart
Understanding the neurobiology of love and loss does not dehumanize these experiences; it gives us the map to navigate them. Recognizing that our brains process attachment through the same reward circuitry as addiction allows us to treat ourselves and others with profound compassion.As we stand on the cusp of being able to pharmacologically “silence” the agony of a broken heart, we face a fundamental question of our identity. The Nirvana Principle seeks the peace of a silenced psyche, yet it is the “excruciating passion” of our attachments that defines the human narrative. We must ask ourselves: If we could take a pill to erase the pain of a breakup by silencing our neural reward systems, would the resulting “tranquility” be worth the loss of the very intensity that makes us human?